Avascular necrosis of the femoral head (AVN) is an increasingly common cause of musculoskeletal disability, and it poses a major diagnostic and therapeutic challenge. Although patients are initially asymptomatic, AVN usually progresses to joint destruction, requiring total hip replacement (THR), usually before the fifth decade. It is estimated that almost 10% of the nearly 500,000 THRs performed each year in the United States are intended to treat AVN; at a cost of more than 1 billion dollars, THRs performed to treat AVN constitute approximately 25% of the total national costs for THR.
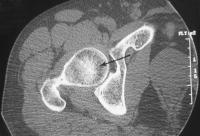
Axial CT in a patient without avascular necrosis of the femoral head shows prominent and thickened but normal trabeculae (arrow) within the femoral head. Note the delicate, sclerotic, raylike branchings emanating in a radial fashion from the central dense band. This is the asterisk sign.
Avascular necrosis, femoral head. Anteroposterior view of the pelvis shows flattening of the outer portion of the right femoral head from avascular necrosis (arrow), with adjacent joint space narrowing, juxta-articular sclerosis, and osteophytes representing degenerative joint disease.
Avascular necrosis, femoral head. Coronal T1-weighted MRI in a patient showing hypointense signal within the proximal femoral neck and intertrochanteric regions (arrows) representing hematopoietic marrow. Increased signal is present within the greater trochanters and femoral capital epiphysis representing normal fatty marrow .
Abdominal CT versus X-Ray Organ doses of radiation from CT scanning are considerably larger than those from corresponding conventional radiography. A conventional anterior-posterior abdominal x-ray examination results in a dose to the stomach of approximately 0.25 mGy, which is at least 50 times smaller than the corresponding stomach dose from an abdominal CT scan. A posterior-anterior chest x-ray would result in a radiation dose to the lungs of 0.01 mGy and a lateral chest x-ray, of a radiation dose of 0.15 mGy to the lungs. Morning Report Questions
Q: Why are more children undergoing diagnostic testing with CT scanning? A: The major growth area in CT use for children has been for the presurgical diagnosis of appendicitis, for which CT appears to be both accurate and cost-effective — though usually no more so than ultrasonography. A considerable literature questions the use of CT, particularly as a primary diagnostic tool for acute appendicitis in children. A poll of pediatric radiologists (Slovis, Pediatr Radiol, 2002) suggested that perhaps one third of all CT studies could be replaced by alternative approaches or not performed at all.
Q: What is a gray (Gy) — the unit used to describe the radiation dose delivered by a CT scan? A: Various measures are used to describe the radiation delivered by CT scanning, the most relevant being absorbed dose, effective dose, and CT dose index. The absorbed dose is the energy absorbed per unit of mass and is measured in grays (Gy). One gray equals 1 joule of radiation energy absorbed per kilogram.
A 46-year-old woman presented with a history of 3 days of pruritus in the anal area and 1 day of excretion of tapelike materials. During the year before presentation, she had reported intermittent colicky abdominal pain and loose stool, which had been attributed to irritable bowel syndrome. Laboratory evaluation was unremarkable, with no evidence of anemia. Colonoscopy revealed a long, moving tapeworm, Diphyllobothrium latum, located in the terminal ileum and extending to the sigmoid colon.
D. latum is a fish tapeworm that can infect humans after they consume infected undercooked or raw fish. The patient had a history of eating raw fish and recalled eating raw trout most recently 2 months before presentation. She was treated with a single dose of praziquantel. After administration, the abdominal pain resolved, but she continued to have intermittent loose stool.
A 59-year-old man presents to the emergency department (ED) complaining of new onset chest pain that radiates to his left arm. He has a historyof hypertension, hypercholesterolemia, and a 20-pack-year smoking history. His ECG is remarkable for T-wave inversions in the lateral leads. Which of the following is the most appropriate next step in management?
a.Give the patient two nitroglycerin tablets sublingually and observe if his chest pain resolves b.Place the patient on a cardiac monitor, administer oxygen, and give aspirin c.Call the cardiac catherization lab for immediate percutaneous intervention (PCI) d.Order a chest x-ray, administer aspirin, clopidogrel, and heparin e.Start a b-blocker immediately
The answer : 1. The answer is b. The patient’s presentation is classic for an ACS. He has multiple risk factorswith T-wave abnormalities on his ECG. The most appropriate initial management includes placing the patient on a cardiac monitor to detect dysrhythmias, establish intravenous access, provide supplemental oxygen, and administer aspirin. If the patient is having active chest pain in the ED, sublingual nitroglycerin or morphine should be administered until the pain resolves. This decreases wall tension and myocardial oxygen demand. A common mnemonic used is that MONA (morphine, oxygen, nitroglycerin, aspirin) greets chest pain patients at the door. (a) Although nitroglycerin is one of the early agents used in ACS, it is prudent to first rule out a right ventricular infarct, which if present, may lead to hypotension. (c)Percutaneous intervention (PCI) is warranted if the patient’s ECG showed ST-segment elevation. (d) The patient will require a chest x-ray and most likely receive clopidogrel and heparin; however this is done only after being on a monitor with oxygen and chewing an aspirin. (e) b-Blockers are usually added for tachycardia, hypertension, and persistent pain and only given once the patient is evaluated for contraindications. Relative contraindications to the use of b-blockers include asthma or chronic obstructive lung disease, CHF, and third-trimester pregnancy
Lymph Nodes: The major lymph node groups are located along the anterior and posterior aspects of the neck and on the underside of the jaw. If the nodes are quite big, you may be able to see them bulging under the skin, particularly if the enlargement is asymmetric (i.e. it will be more obvious if one side is larger then the other). To palpate, use the pads of all four fingertips as these are the most sensitive parts of your hands. Examine both sides of the head simultaneously, walking your fingers down the area in question while applying steady, gentle pressure. The major groups of lymph nodes as well as the structures that they drain, are listed below. The description of drainage pathways are rough approximations as there is frequently a fair amount of variability and overlap. Nodes are generally examined in the following order: 1. Anterior Cervical (both superficial and deep): Nodes that lie both on top of and beneath the sternocleidomastoid muscles (SCM) on either side of the neck, from the angle of the jaw to the top of the clavicle. This muscle allows the head to turn to the right and left. The right SCM turns the head to the left and vice versa. They can be easily identified by asking the patient to turn their head into your hand while you provide resistance. Drainage: The internal structures of the throat as well as part of the posterior pharynx, tonsils, and thyroid gland.
2. Posterior Cervical: Extend in a line posterior to the SCMs but in front of the trapezius, from the level of the mastoid bone to the clavicle. Drainage: The skin on the back of the head. Also frequently enlarged during upper respiratory infections (e.g. mononucleosis). 3. Tonsillar: Located just below the angle of the mandible. Drainage: The tonsilar and posterior pharyngeal regions. 4. Sub-Mandibular: Along the underside of the jaw on either side. Drainage: The structures in the floor of the mouth. 5. Sub-Mental: Just below the chin. Drainage: The teeth and intra-oral cavity. 6. Supra-clavicular: In the hollow above the clavicle, just lateral to where it joins the sternum. Drainage: Part of the throacic cavity, abdomen.
Increased Anterior Posterior Diameter: Barrel chested appearance resulting from air trapping that sometimes occurs with advanced COPD. Xray on the right also demonstrates the increased A-P diameter along with flattening of the diaphragms.
Spanish surgeons have announced that they have carried out the world's first full-face transplant.
The hospital, in Barcelona, performed the surgery on a young man who lost his face in an accident five years ago. Since then, he'd been unable to swallow, speak or breathe properly.
A 55-year-old man presents with a history of hypertension that is becoming more diffi cult to control despite the use of three antihypertensive drugs over the last two years. Clinical examination reveals a vascular bruit in the region of the right kidney. Renal function is normal. An MR angiogram of the renal arteries was performed..
Right Answer :Renal artery stenosis- The right kidney is signifi cantly smaller than the left. - There is ostial stenosis of the right renal artery.
Actinic keratosis is a precancerous skin growth usually caused by sun exposure.
Actinic keratosis occurs most commonly in fair skin, especially in the elderly and in young individuals with light complexions. The growths occur in sun-exposed skin areas. The growths begin as flat scaly areas that later develop a hard wart-like surface.
They are classified as precancerous growths. If left untreated, approximately 10% of actinic keratoses develop into squamous cell carcinoma.
Adenoid Cystic Carcinoma is a type of cancer characterized by large epithelial masses containing round glandlike spaces or cysts, frequently containing mucus, that are bordered by layers of
As the strongest tendon of the human body, the Achilles tendon originates from the soleus and gastrocnemius muscles, and inserts onto the posterior calcaneal tuberosity. The tendon is surrounded by a paratenon rather than a synovial sheath. Sonography is an efficient and accurate way to assess the Achilles tendon. Advantages of sonographic evaluation include cost, widely available equipment, ease of contralateral comparison, and the ability to image during joint motion.
Post exposure HIV prophylaxis is recommended if there is:-
* unprotected receptive anal intercourse
* unprotected receptive vaginal intercourse
* unprotected insertive vaginal intercourse
* unprotected insertive anal intercourse
* unprotected receptive fellatio with ejaculation
with a HIV positive person or if the person is a HIV risk group (gay or bisexual men, injection drug users or sex workers), and if the exposure is isolated and the patient is commited to safer sex in the future and the exposure occurred within 72 hours of presentation for care.
Exposure to persons known to be HIV infected
if medication regimen of source patient is unknown => prescribe Zivudine (AZT/ZDV) 300mg bid + Lamivudine (Epivir) 150mg bid + Indinavir (Crixivan) 800mh q8h or nelfinavir (Virasept) 1250mg bid or 750mg tid
Combivir 1 tablet bid may be substituted for zidovudine and lamivudine
if medication regimen of source patient is known => prescribe 2 NRTIs and 1 protease inhibitor that are different from the source patient's regimen
possible substitues for zidovudine and lamivudine:- stavudine (d4T/Zerit) 40mg bid for > 60kg and 30mg bid <> 60kg and 125mg for <>
Exposure to person or persons of unknown HIV status but who probably have high HIV risk factors :
significant exposures => treat as if an exposure to a known HIV-infected person with an unknown medication regimen, as above
exposures that might result in HIV infection => treat with zidovudine and lamivudine without a protease inhibitor
Exposure to person or persons of unknown HIV status but who probably have low HIV risk factors
significant exposures => treat with zidovudine and lamivudine. A protease inhibitor could be added if the patient requests it, if the provider believes that the exposure history is unclear, other exposures also occurred, or if other factors relating to exposure history or HIV status are compelling
exposures that might result in HIV infection => treat with zidovudine and lamivudine without a protease inhibitor
Additional caveats
* PEP should not be provided to patients whose exposure history has no known possibility for HIV transmission
* PEP should not be given to persons already infected with HIV
* providers may consider PEP for any patient who appears to be at risk after an HIV exposure but whose circumstances are not delineated in the above categories
Providers are reminded that PEP should only be prescribed as part of a comprehensive program to reduce future HIV risk-related behaviours. Multiple prescription requests for PEP should be strongly discouraged and must be averted through risk reduction counselling.
Definitions:
High HIV risk factors: trading sex for drugs or money, IV drug use, unprotected anal or vaginal intercourse with persons with HIV risk factors
Significant exposures include the following: anal or vaginal intercourse without a condom or with condom breakage; exposure to semen or blood onto mucosal or nonintact surfaces, and intravenous needle sharing
Examples of exposures that might result in HIV infection are as follows: cunnilingus, fellatio, semen or blood on healing skin wounds
Transurethral catheters (Foley catheters) have one-way, two-way or three-way variations. The one-way catheter is a simple tube used to remove urine without securing the tube. This is used when someone is "straight catheterized." The two-way tubing has an outlet for urine and a conduit for water inflation of the catheter's balloon. This is the most commonly used catheter. The three-way tubing has an outlet for urine, an inlet for water inflation of the balloon, and an inlet for normal saline used for irrigating the urinary system most commonly for gross hematuria. There also exist whistle-tipped and multi-eyed variations. These tubes have larger and more draining holes, respectively, and are useful when blood clots are present. Most catheters are made of silicon, which is smoother than latex. Silicon catheters should be used in patients with an allergy to latex.
In order to obtain financial help with diabetes medicine, it's important to have health insurance or to look into government-regulated programs. Learn about drug companies that will give medication at a discounted price with help from a licensed RN in this free video on diabetes medicine.
A 37-year-old man with a history of spina bifida presented with an audible knocking sound coming from his abdomen during ambulation. Fifteen years earlier he had undergone a cystectomy with a continent cutaneous urinary diversion (Indiana pouch) for a neurogenic bladder. He had been poorly compliant with the catheterization and irrigation regimen involving the pouch.
Physical examination revealed a well-healed, functional stoma and a palpable mass in the right side of the abdomen. Urinalysis revealed a urinary pH of 9.0, with numerous white and red cells, and urine culture grew Proteus mirabilis.
Plain abdominal radiography revealed two large multilaminar calcifications in the right side of the abdomen (Panel A). Computed tomography of the abdomen and pelvis confirmed the presence of two large calculi within the Indiana pouch (Panel B). The patient underwent cystolithotomy without incident. At a follow-up visit 1 year after the procedure, he was found to have been compliant with his catheterization and irrigation regimen and remained free of stones.
Continent urinary diversions may be associated with hypercalciuria, hyperphosphaturia, hyperoxaluria, and hypocitraturia, all of which may predispose patients to pouch urolithiasis. Infections with organisms that break down urea can result in an alkaline environment, which can in turn give rise to struvite (magnesium ammonium phosphate) stones. Establishment of a formal catheterization and irrigation protocol for continent urinary diversions may reduce the risk of urolithiasis.
A one year old old boy with known renal failure presents is brought to Casualty after a seizure. He is noted to have marked bowing of the long bones of his lower limbs. An xray of the lower limbs shows cupping, fraying and irregularity of the metaphyses.
The Atlas of Minor Oral Surgery is a striking, highly illustrated reference book that is tailor-made for the general dentist who wants to expand the services offered in the dental office. This book is a definitive resource on both clinical and patient management aspects of outpatient minor oral surgery as the dentist can learn how to perform oral and surgical techniques that he or she previously referred to the oral surgeon.
Ehlers-Danlos syndrome (EDS) is the name given to a group of more than 10 different inherited disorders; all involve a genetic defect in collagen and connective-tissue synthesis and structure.
Ehlers-Danlos syndrome can affect the skin, joints, and blood vessels. This syndrome is clinically heterogeneous; the underlying collagen abnormality is different for each type. Clinical recognition of the types of Ehlers-Danlos syndrome is important. One type, type IV, is associated with arterial rupture and visceral perforation, with possible life-threatening consequences.
Clinical:
History
The biochemical collagen defect is present at birth, but clinical manifestations become evident later.
1- Muscle weakness is often present, and patients report a tendency to fall down easily and have poor body control.
2-Sometimes, patients have difficulty walking.
3-Mental development is normal.
4- The newly described tenascin-X–deficient form was described in 8 patients with hyperelastic skin and hypermobile joints.
* Each patient bruised easily, and most had velvety skin.
* A few patients also had joint pain and multiple subluxations.
* None had delayed wound healing or atrophic scars.
* Additional findings in some patients included congenital adrenal hyperplasia, mitral valvular prolapse, stroke, gut bleeding, and premature arteriosclerosis.
5- Dental pathology is common in these patients. Findings include hypodontia of permanent teeth, delayed eruption, and dentin dysplasia.
6-In one patient, splenic rupture due to peliosis led to the diagnosis of vascular Ehlers-Danlos syndrome.
7- Multiple sclerosis can be associated with Ehlers-Danlos syndrome.
8- Absence of the inferior labial or lingual frenula in Ehlers-Danlos syndrome patients has been suggested as a new diagnostic criterion.
9-Ehlers-Danlos syndrome and anorexia nervosa have been described in the same patient.
Physical
To date, 11 variants of Ehlers-Danlos syndrome are identified; all have genetic, biochemical, and clinical differences. More than one third of persons with Ehlers-Danlos syndrome do not fit exactly into a single type; overlap is common.
* Common to almost all groups is a unique appearance of the skin.
The skin is usually white and soft, and underlying vessels are sometimes visible.
The skin has a doughy feel.
The skin is easily hyperextensible. It is easy to pull, and, once released, it immediately returns to its original state.
* Molluscoid pseudotumors are small, spongy tumors found over scars and pressure points.
Molluscoid pseudotumors consist of fat surrounded by a fibrous capsule.
They are commonly seen in patients with type I.
* Smaller, deep, palpable, and movable nodules are often present in the subcutaneous tissue.
These nodules can be found in the arms and over the tibias.
Calcification leads to opacity on radiographs.
* Fragility of dermal skin is common, with frequent bruises and lacerations.
Poor wound healing is not rare.
The use of sutures is usually a problem in patients, in whom easy dehiscence and cigarette-paper–like scars may be observed. Frequently, these scars are found on the knees.
* The joints are hyperextensible, sometimes dramatically, but the degree of involvement is variable.
The digit joints are most commonly affected, but all the joints can show alterations.
Dislocations can occur, but patients are usually able to quickly reduce them with no pain.
A condition characterized by a smooth, glossy, erythematous, edematous tongue that is generally painful.
The tongue appears smooth because of loss of filiform and fungiform papillae. This condition occurs during a vitamin B deficiency, such as in pellagra, and certain disorders like pernicious anemia.
Circumferential pelvic anti-shock sheeting. A. A sheet is placed under the pelvis. B. The ends are brought together anteriorly. C. Hemostats are used to secure the sheet snugly.
* A simple method for obtaining temporary pelvic stabilization when an external fixator cannot be applied is the application of a circumferential pelvic anti-shock sheet (CPAS). * Advantages of this technique include the fact that it is inexpensive and readily available in all EDs. Special training is not required and the emergency physician can apply the sheet. Lower extremity and abdominal access is maintained after the sheet is placed. * Caution is required in patients with lateral compression pelvic ring injuries or sacral neuroforaminal fractures. Forceful or aggressive CPAS application could worsen visceral injury or sacral nerve root injury in these instances.
On mammography , male breast cancer is subareolar or somewhat eccentric to the nipple, with well-defined, ill-defined, or spiculated margins. Calcifications are observed less commonly than in female breast cancer and, when found, are coarser in appearance. Calcifications can also be seen in fat necrosis. Axillary adenopathy may be observed as well.
Mammography is highly sensitive and specific for breast cancer in men, but it should be used to complement the clinical examination. At present, not enough clinical data are available to determine whether the combination of imaging and clinical findings can replace biopsy for the diagnosis of palpable breast abnormalities in men. Ultimately, biopsy should be considered to diagnose male breast cancer because the findings of inflammation, gynecomastia, and fat necrosis can be similar.
False Positives/Negatives
Inflammation, gynecomastia, and fat necrosis may appear similar on mammograms; therefore, these condition can cause false-positive findings. Cases of carcinoma have been found by ultrasonography after they were obscured on previous mammograms by gynecomastia.
A partially circumscribed retroareolar mass in a male with suspicious microcalcifications; this is known breast cancer.
Findings on Ultrasonography:
A hypoechoic mass with irregular, ill-defined, or circumscribed margins may be observed on ultrasonography. With color flow imaging, vascular flow within the mass may be demonstrated.
Similar sonographic findings may be observed in gynecomastia or inflammation; therefore, ultrasonography alone is not a reliable method to distinguish male breast cancer from other etiologies.
1-Supernumerary Nipple,Accessory Nipple, Polythelia,Ectopic nipple, Extra nipple, Hyperthelia.
2- Usually develop along the course of the embryological milk lines, which run from the anterior axillary folds to the inner thighs, but may also occur in other sites.
Acrocyanosis of the hands and feet commonly seen in newborns.
Acrocyanosis: Bluish discoloration of the extremities (the hands and feet). Acrocyanosis is typically symmetrical. It is marked by a mottled blue or red discoloration of the skin of the fingers and wrists and the toes and ankles and by profuse sweating and coldness of the fingers and toes.
Acrocyanosis is caused by narrowing (constriction) of small arterioles (tiny arteries) toward the end of the arms and legs.
c. Atelectasis of the left lung because of a mucus plug
d. Pneumonia in the left lung
e. Atelectasis of the left lung because the ETT is too low
Correct Answer:
Atelectasis of the left lung because the ETT is too low
Explanation
There is opacification of the left hemithorax. There is a shift of the heart and mediastinal structures (i.e. the trachea) toward the side of opacification. This eliminates pleural effusion, pneumonia and pulmonary edema as possibilities. A tension pneumothorax will displace the heart and mediastinal structures away from the side of the pneumothorax but it will not cause complete opacification of the opposite lung. In addition, there should be no lung markings visible in the hemithorax which contains the pneumothorax. If you look carefully, you will see the markers on an endotracheal tube that extends into the right mainstem bronchus. Thus, only the right lung is being aerated and the left lung has become atelectatic.
Salter-Harris fractures are fractures through a growth plate; therefore, they are unique to pediatric patients. Several types of fractures have been categorized by the involvement of the physis, metaphysis, and epiphysis. The classification of the injury is important because it affects the treatment of the patient and provides clues to possible long-term complications. * Type I - fracture through the physis (widened physis) * Type II - fracture partway through the physis extending up into metaphysis * Type III - fracture partway through the physis extending down into the epiphysis * Type IV - fracture through the metaphysis, physis, and epiphysis -- can lead to angulation deformities when healing * Type V - crush injury to the physis
No validated rules have been formulated for the use of radiography in patients with suspected ligament injuries, but a decision tree can be used as a guide (Figure below). Although plain radiographs may be useful in the initial diagnosis of these injuries, magnetic resonance imaging (MRI) is becoming the preferred diagnostic method and is rapidly replacing other techniques as the study of choice for the evaluation of knee injuries. However, the routine use of MRI has been questioned because of its significant cost ($600 to $1,200) and the high accuracy of clinical examination in diagnosing some injuries.
A knee x-ray is only required for knee injury patients with any of these findings:
age 55 or over
isolated tenderness of the patella (no bone tenderness of the knee other than the patella)
tenderness at the head of the fibula
inability to flex to 90 degrees
inability to weight bear both immediately and in the casualty department (4 steps - unable to transfer weight twice onto each lower limb regardless of limping)
A 31-year-old Caucasian male is admitted to the hospital with a 10-day history lower extremities rash and hands and feet swelling. He had upper respiratory tract infection before his current symptoms started.
A biopsy of skin lesions at an outside hospital shows leukoclastic vasculitis. All his other laboratory results are normal, including ESR, CRP, UA, CBC, CMP.
He received Celecoxib (Celebrex) 200 mg po daily started 5 days ago.Past medical history was Negative.
Physical examination:
Afebrile,well-developed and well-nourished
Chest: CTA (B).
CVS: Clear S1S2.
Abdomen: Soft, NT, ND, +BS.
Extremities: edema of hands and feet , purpura of lower extremities.
Edema of hands and feet
Purpura and edema of lower extremities
CBC, CMP, UA, ESR, CRP are all normal.
X-rays of hands are normal.
the likely diagnosis:Henoch-Schönlein Purpura
test to help confirm the diagnosis:
IgA
ASO
Throat culture
GC/Chlamydia probe
Stool guaiac
Results:
IgA level was elevated: IgA 516 mg/dL (lower limit 78, upper limit 391). ASO was elevated but the the throat culture was negative. The rest of the tests were normal.
Rheumatology and ID consults confirmed the diagnosis of Henoch-Schönlein purpura.
On hospital day 2, the purpura and swelling started to resolve. The patient felt much better and was discharged home with Celecoxib (Celebrex) 200 mg po qd and follow-up with rheumatology in 3-4 weeks. He was scheduled to have UA and BMP at that time to monitor for development of HSP-related renal disease.
What did we learn from this case?
Henoch-Schönlein purpura (HSP) is a self-limited systemic vasculitis. It is characterized by 4 clinical syndromes:
1. Palpable purpura in the absence of thrombocytopenia or coagulopathy. Develops in 100% of patients.
2. Arthritis/arthralgia in 45-75% of patients. Second most common manifestation of HSP.
3. Abdominal pain in 50%, GI bleeding (often occult) in 20-30% of patients.
A 65-year-old man collapses and is brought into the casualty department. Chest X-ray shows an increase in the cardiothoracic ration but clear lung fields. He is found to have decreased arterial pressure, increased central venous pressure, and faint heart sounds .
What is the most likely diagnosis?
a) Cardiogenic shock
b)Mitral regurgitation
c) Pericardial tamponade
d) Pulmonary embolism
e) Ventricular septal defect
The correct answer is C
Explanation
Pericardial tamponade classically results in the acute cardiac compression triad of Beck, which consists of decreased arterial pressure, increased central venous pressure, and distant heart sounds . Although clearly pathognomonic for tamponade, Beck's triad occurs in only 10% of individuals with pericardial tamponade
To keep it cool during hot-weather exercise, keep these basic precautions in mind:
* Take it slow . If you're used to exercising indoors or in cooler weather, take it easy at first. As your body adapts to the heat, gradually increase the length and intensity of your workouts. If you have a chronic medical condition or take medication, ask your doctor if you need to take additional precautions.
* Drink plenty of fluids . Your body's ability to sweat and cool down depends on adequate rehydration. Drink plenty of water while you're working out — even if you don't feel thirsty. If you're planning to exercise intensely or for longer than one hour, consider sports drinks instead. These drinks can replace the sodium, chloride and potassium you lose through sweating. Avoid drinks that contain caffeine or alcohol, which actually promote fluid loss.
* Dress appropriately . Lightweight, loosefitting clothing promotes sweat evaporation and cooling by letting more air pass over your body. Avoid dark colors, which can absorb the heat. A light-colored hat can limit your exposure to the sun.
* Avoid midday sun . Exercise in the morning or evening — when it's likely to be cooler outdoors — rather than the middle of the day. If possible, exercise in the shade or in a pool.
* Wear sunscreen . A sunburn decreases your body's ability to cool itself.
* Have a backup plan . If you're concerned about the heat or humidity, stay indoors. Work out at the gym, walk laps inside the mall or climb stairs inside an air-conditioned building.
Avascular necrosis of the femoral head (AVN) is an increasingly common cause of musculoskeletal disability, and it poses a major diagnostic and therapeutic challenge. Although patients are initially asymptomatic, AVN usually progresses to joint destruction, requiring total hip replacement (THR), usually before the fifth decade. It is estimated that almost 10% of the nearly 500,000 THRs performed each year in the United States are intended to treat AVN; at a cost of more than 1 billion dollars, THRs performed to treat AVN constitute approximately 25% of the total national costs for THR.
Axial CT in a patient without avascular necrosis of the femoral head shows prominent and thickened but normal trabeculae (arrow) within the femoral head. Note the delicate, sclerotic, raylike branchings emanating in a radial fashion from the central dense band. This is the asterisk sign.
Avascular necrosis, femoral head. Anteroposterior view of the pelvis shows flattening of the outer portion of the right femoral head from avascular necrosis (arrow), with adjacent joint space narrowing, juxta-articular sclerosis, and osteophytes representing degenerative joint disease.
Avascular necrosis, femoral head. Coronal T1-weighted MRI in a patient showing hypointense signal within the proximal femoral neck and intertrochanteric regions (arrows) representing hematopoietic marrow. Increased signal is present within the greater trochanters and femoral capital epiphysis representing normal fatty marrow .
Abdominal CT versus X-Ray Organ doses of radiation from CT scanning are considerably larger than those from corresponding conventional radiography. A conventional anterior-posterior abdominal x-ray examination results in a dose to the stomach of approximately 0.25 mGy, which is at least 50 times smaller than the corresponding stomach dose from an abdominal CT scan. A posterior-anterior chest x-ray would result in a radiation dose to the lungs of 0.01 mGy and a lateral chest x-ray, of a radiation dose of 0.15 mGy to the lungs. Morning Report Questions
Q: Why are more children undergoing diagnostic testing with CT scanning? A: The major growth area in CT use for children has been for the presurgical diagnosis of appendicitis, for which CT appears to be both accurate and cost-effective — though usually no more so than ultrasonography. A considerable literature questions the use of CT, particularly as a primary diagnostic tool for acute appendicitis in children. A poll of pediatric radiologists (Slovis, Pediatr Radiol, 2002) suggested that perhaps one third of all CT studies could be replaced by alternative approaches or not performed at all.
Q: What is a gray (Gy) — the unit used to describe the radiation dose delivered by a CT scan? A: Various measures are used to describe the radiation delivered by CT scanning, the most relevant being absorbed dose, effective dose, and CT dose index. The absorbed dose is the energy absorbed per unit of mass and is measured in grays (Gy). One gray equals 1 joule of radiation energy absorbed per kilogram.
A 46-year-old woman presented with a history of 3 days of pruritus in the anal area and 1 day of excretion of tapelike materials. During the year before presentation, she had reported intermittent colicky abdominal pain and loose stool, which had been attributed to irritable bowel syndrome. Laboratory evaluation was unremarkable, with no evidence of anemia. Colonoscopy revealed a long, moving tapeworm, Diphyllobothrium latum, located in the terminal ileum and extending to the sigmoid colon.
D. latum is a fish tapeworm that can infect humans after they consume infected undercooked or raw fish. The patient had a history of eating raw fish and recalled eating raw trout most recently 2 months before presentation. She was treated with a single dose of praziquantel. After administration, the abdominal pain resolved, but she continued to have intermittent loose stool.
A 59-year-old man presents to the emergency department (ED) complaining of new onset chest pain that radiates to his left arm. He has a historyof hypertension, hypercholesterolemia, and a 20-pack-year smoking history. His ECG is remarkable for T-wave inversions in the lateral leads. Which of the following is the most appropriate next step in management?
a.Give the patient two nitroglycerin tablets sublingually and observe if his chest pain resolves b.Place the patient on a cardiac monitor, administer oxygen, and give aspirin c.Call the cardiac catherization lab for immediate percutaneous intervention (PCI) d.Order a chest x-ray, administer aspirin, clopidogrel, and heparin e.Start a b-blocker immediately
The answer : 1. The answer is b. The patient’s presentation is classic for an ACS. He has multiple risk factorswith T-wave abnormalities on his ECG. The most appropriate initial management includes placing the patient on a cardiac monitor to detect dysrhythmias, establish intravenous access, provide supplemental oxygen, and administer aspirin. If the patient is having active chest pain in the ED, sublingual nitroglycerin or morphine should be administered until the pain resolves. This decreases wall tension and myocardial oxygen demand. A common mnemonic used is that MONA (morphine, oxygen, nitroglycerin, aspirin) greets chest pain patients at the door. (a) Although nitroglycerin is one of the early agents used in ACS, it is prudent to first rule out a right ventricular infarct, which if present, may lead to hypotension. (c)Percutaneous intervention (PCI) is warranted if the patient’s ECG showed ST-segment elevation. (d) The patient will require a chest x-ray and most likely receive clopidogrel and heparin; however this is done only after being on a monitor with oxygen and chewing an aspirin. (e) b-Blockers are usually added for tachycardia, hypertension, and persistent pain and only given once the patient is evaluated for contraindications. Relative contraindications to the use of b-blockers include asthma or chronic obstructive lung disease, CHF, and third-trimester pregnancy
Lymph Nodes: The major lymph node groups are located along the anterior and posterior aspects of the neck and on the underside of the jaw. If the nodes are quite big, you may be able to see them bulging under the skin, particularly if the enlargement is asymmetric (i.e. it will be more obvious if one side is larger then the other). To palpate, use the pads of all four fingertips as these are the most sensitive parts of your hands. Examine both sides of the head simultaneously, walking your fingers down the area in question while applying steady, gentle pressure. The major groups of lymph nodes as well as the structures that they drain, are listed below. The description of drainage pathways are rough approximations as there is frequently a fair amount of variability and overlap. Nodes are generally examined in the following order: 1. Anterior Cervical (both superficial and deep): Nodes that lie both on top of and beneath the sternocleidomastoid muscles (SCM) on either side of the neck, from the angle of the jaw to the top of the clavicle. This muscle allows the head to turn to the right and left. The right SCM turns the head to the left and vice versa. They can be easily identified by asking the patient to turn their head into your hand while you provide resistance. Drainage: The internal structures of the throat as well as part of the posterior pharynx, tonsils, and thyroid gland.
2. Posterior Cervical: Extend in a line posterior to the SCMs but in front of the trapezius, from the level of the mastoid bone to the clavicle. Drainage: The skin on the back of the head. Also frequently enlarged during upper respiratory infections (e.g. mononucleosis). 3. Tonsillar: Located just below the angle of the mandible. Drainage: The tonsilar and posterior pharyngeal regions. 4. Sub-Mandibular: Along the underside of the jaw on either side. Drainage: The structures in the floor of the mouth. 5. Sub-Mental: Just below the chin. Drainage: The teeth and intra-oral cavity. 6. Supra-clavicular: In the hollow above the clavicle, just lateral to where it joins the sternum. Drainage: Part of the throacic cavity, abdomen.
Increased Anterior Posterior Diameter: Barrel chested appearance resulting from air trapping that sometimes occurs with advanced COPD. Xray on the right also demonstrates the increased A-P diameter along with flattening of the diaphragms.
Spanish surgeons have announced that they have carried out the world's first full-face transplant.
The hospital, in Barcelona, performed the surgery on a young man who lost his face in an accident five years ago. Since then, he'd been unable to swallow, speak or breathe properly.
A 55-year-old man presents with a history of hypertension that is becoming more diffi cult to control despite the use of three antihypertensive drugs over the last two years. Clinical examination reveals a vascular bruit in the region of the right kidney. Renal function is normal. An MR angiogram of the renal arteries was performed..
Right Answer :Renal artery stenosis- The right kidney is signifi cantly smaller than the left. - There is ostial stenosis of the right renal artery.
Actinic keratosis is a precancerous skin growth usually caused by sun exposure.
Actinic keratosis occurs most commonly in fair skin, especially in the elderly and in young individuals with light complexions. The growths occur in sun-exposed skin areas. The growths begin as flat scaly areas that later develop a hard wart-like surface.
They are classified as precancerous growths. If left untreated, approximately 10% of actinic keratoses develop into squamous cell carcinoma.
Adenoid Cystic Carcinoma is a type of cancer characterized by large epithelial masses containing round glandlike spaces or cysts, frequently containing mucus, that are bordered by layers of
As the strongest tendon of the human body, the Achilles tendon originates from the soleus and gastrocnemius muscles, and inserts onto the posterior calcaneal tuberosity. The tendon is surrounded by a paratenon rather than a synovial sheath. Sonography is an efficient and accurate way to assess the Achilles tendon. Advantages of sonographic evaluation include cost, widely available equipment, ease of contralateral comparison, and the ability to image during joint motion.
Post exposure HIV prophylaxis is recommended if there is:-
* unprotected receptive anal intercourse
* unprotected receptive vaginal intercourse
* unprotected insertive vaginal intercourse
* unprotected insertive anal intercourse
* unprotected receptive fellatio with ejaculation
with a HIV positive person or if the person is a HIV risk group (gay or bisexual men, injection drug users or sex workers), and if the exposure is isolated and the patient is commited to safer sex in the future and the exposure occurred within 72 hours of presentation for care.
Exposure to persons known to be HIV infected
if medication regimen of source patient is unknown => prescribe Zivudine (AZT/ZDV) 300mg bid + Lamivudine (Epivir) 150mg bid + Indinavir (Crixivan) 800mh q8h or nelfinavir (Virasept) 1250mg bid or 750mg tid
Combivir 1 tablet bid may be substituted for zidovudine and lamivudine
if medication regimen of source patient is known => prescribe 2 NRTIs and 1 protease inhibitor that are different from the source patient's regimen
possible substitues for zidovudine and lamivudine:- stavudine (d4T/Zerit) 40mg bid for > 60kg and 30mg bid <> 60kg and 125mg for <>
Exposure to person or persons of unknown HIV status but who probably have high HIV risk factors :
significant exposures => treat as if an exposure to a known HIV-infected person with an unknown medication regimen, as above
exposures that might result in HIV infection => treat with zidovudine and lamivudine without a protease inhibitor
Exposure to person or persons of unknown HIV status but who probably have low HIV risk factors
significant exposures => treat with zidovudine and lamivudine. A protease inhibitor could be added if the patient requests it, if the provider believes that the exposure history is unclear, other exposures also occurred, or if other factors relating to exposure history or HIV status are compelling
exposures that might result in HIV infection => treat with zidovudine and lamivudine without a protease inhibitor
Additional caveats
* PEP should not be provided to patients whose exposure history has no known possibility for HIV transmission
* PEP should not be given to persons already infected with HIV
* providers may consider PEP for any patient who appears to be at risk after an HIV exposure but whose circumstances are not delineated in the above categories
Providers are reminded that PEP should only be prescribed as part of a comprehensive program to reduce future HIV risk-related behaviours. Multiple prescription requests for PEP should be strongly discouraged and must be averted through risk reduction counselling.
Definitions:
High HIV risk factors: trading sex for drugs or money, IV drug use, unprotected anal or vaginal intercourse with persons with HIV risk factors
Significant exposures include the following: anal or vaginal intercourse without a condom or with condom breakage; exposure to semen or blood onto mucosal or nonintact surfaces, and intravenous needle sharing
Examples of exposures that might result in HIV infection are as follows: cunnilingus, fellatio, semen or blood on healing skin wounds
Read More
Transurethral catheters (Foley catheters) have one-way, two-way or three-way variations. The one-way catheter is a simple tube used to remove urine without securing the tube. This is used when someone is "straight catheterized." The two-way tubing has an outlet for urine and a conduit for water inflation of the catheter's balloon. This is the most commonly used catheter. The three-way tubing has an outlet for urine, an inlet for water inflation of the balloon, and an inlet for normal saline used for irrigating the urinary system most commonly for gross hematuria. There also exist whistle-tipped and multi-eyed variations. These tubes have larger and more draining holes, respectively, and are useful when blood clots are present. Most catheters are made of silicon, which is smoother than latex. Silicon catheters should be used in patients with an allergy to latex.
In order to obtain financial help with diabetes medicine, it's important to have health insurance or to look into government-regulated programs. Learn about drug companies that will give medication at a discounted price with help from a licensed RN in this free video on diabetes medicine.
A 37-year-old man with a history of spina bifida presented with an audible knocking sound coming from his abdomen during ambulation. Fifteen years earlier he had undergone a cystectomy with a continent cutaneous urinary diversion (Indiana pouch) for a neurogenic bladder. He had been poorly compliant with the catheterization and irrigation regimen involving the pouch.
Physical examination revealed a well-healed, functional stoma and a palpable mass in the right side of the abdomen. Urinalysis revealed a urinary pH of 9.0, with numerous white and red cells, and urine culture grew Proteus mirabilis.
Plain abdominal radiography revealed two large multilaminar calcifications in the right side of the abdomen (Panel A). Computed tomography of the abdomen and pelvis confirmed the presence of two large calculi within the Indiana pouch (Panel B). The patient underwent cystolithotomy without incident. At a follow-up visit 1 year after the procedure, he was found to have been compliant with his catheterization and irrigation regimen and remained free of stones.
Continent urinary diversions may be associated with hypercalciuria, hyperphosphaturia, hyperoxaluria, and hypocitraturia, all of which may predispose patients to pouch urolithiasis. Infections with organisms that break down urea can result in an alkaline environment, which can in turn give rise to struvite (magnesium ammonium phosphate) stones. Establishment of a formal catheterization and irrigation protocol for continent urinary diversions may reduce the risk of urolithiasis.
A one year old old boy with known renal failure presents is brought to Casualty after a seizure. He is noted to have marked bowing of the long bones of his lower limbs. An xray of the lower limbs shows cupping, fraying and irregularity of the metaphyses.
The Atlas of Minor Oral Surgery is a striking, highly illustrated reference book that is tailor-made for the general dentist who wants to expand the services offered in the dental office. This book is a definitive resource on both clinical and patient management aspects of outpatient minor oral surgery as the dentist can learn how to perform oral and surgical techniques that he or she previously referred to the oral surgeon.
Ehlers-Danlos syndrome (EDS) is the name given to a group of more than 10 different inherited disorders; all involve a genetic defect in collagen and connective-tissue synthesis and structure.
Ehlers-Danlos syndrome can affect the skin, joints, and blood vessels. This syndrome is clinically heterogeneous; the underlying collagen abnormality is different for each type. Clinical recognition of the types of Ehlers-Danlos syndrome is important. One type, type IV, is associated with arterial rupture and visceral perforation, with possible life-threatening consequences.
Clinical:
History
The biochemical collagen defect is present at birth, but clinical manifestations become evident later.
1- Muscle weakness is often present, and patients report a tendency to fall down easily and have poor body control.
2-Sometimes, patients have difficulty walking.
3-Mental development is normal.
4- The newly described tenascin-X–deficient form was described in 8 patients with hyperelastic skin and hypermobile joints.
* Each patient bruised easily, and most had velvety skin.
* A few patients also had joint pain and multiple subluxations.
* None had delayed wound healing or atrophic scars.
* Additional findings in some patients included congenital adrenal hyperplasia, mitral valvular prolapse, stroke, gut bleeding, and premature arteriosclerosis.
5- Dental pathology is common in these patients. Findings include hypodontia of permanent teeth, delayed eruption, and dentin dysplasia.
6-In one patient, splenic rupture due to peliosis led to the diagnosis of vascular Ehlers-Danlos syndrome.
7- Multiple sclerosis can be associated with Ehlers-Danlos syndrome.
8- Absence of the inferior labial or lingual frenula in Ehlers-Danlos syndrome patients has been suggested as a new diagnostic criterion.
9-Ehlers-Danlos syndrome and anorexia nervosa have been described in the same patient.
Physical
To date, 11 variants of Ehlers-Danlos syndrome are identified; all have genetic, biochemical, and clinical differences. More than one third of persons with Ehlers-Danlos syndrome do not fit exactly into a single type; overlap is common.
* Common to almost all groups is a unique appearance of the skin.
The skin is usually white and soft, and underlying vessels are sometimes visible.
The skin has a doughy feel.
The skin is easily hyperextensible. It is easy to pull, and, once released, it immediately returns to its original state.
* Molluscoid pseudotumors are small, spongy tumors found over scars and pressure points.
Molluscoid pseudotumors consist of fat surrounded by a fibrous capsule.
They are commonly seen in patients with type I.
* Smaller, deep, palpable, and movable nodules are often present in the subcutaneous tissue.
These nodules can be found in the arms and over the tibias.
Calcification leads to opacity on radiographs.
* Fragility of dermal skin is common, with frequent bruises and lacerations.
Poor wound healing is not rare.
The use of sutures is usually a problem in patients, in whom easy dehiscence and cigarette-paper–like scars may be observed. Frequently, these scars are found on the knees.
* The joints are hyperextensible, sometimes dramatically, but the degree of involvement is variable.
The digit joints are most commonly affected, but all the joints can show alterations.
Dislocations can occur, but patients are usually able to quickly reduce them with no pain.
A condition characterized by a smooth, glossy, erythematous, edematous tongue that is generally painful.
The tongue appears smooth because of loss of filiform and fungiform papillae. This condition occurs during a vitamin B deficiency, such as in pellagra, and certain disorders like pernicious anemia.
Circumferential pelvic anti-shock sheeting. A. A sheet is placed under the pelvis. B. The ends are brought together anteriorly. C. Hemostats are used to secure the sheet snugly.
* A simple method for obtaining temporary pelvic stabilization when an external fixator cannot be applied is the application of a circumferential pelvic anti-shock sheet (CPAS). * Advantages of this technique include the fact that it is inexpensive and readily available in all EDs. Special training is not required and the emergency physician can apply the sheet. Lower extremity and abdominal access is maintained after the sheet is placed. * Caution is required in patients with lateral compression pelvic ring injuries or sacral neuroforaminal fractures. Forceful or aggressive CPAS application could worsen visceral injury or sacral nerve root injury in these instances.
Read More
On mammography , male breast cancer is subareolar or somewhat eccentric to the nipple, with well-defined, ill-defined, or spiculated margins. Calcifications are observed less commonly than in female breast cancer and, when found, are coarser in appearance. Calcifications can also be seen in fat necrosis. Axillary adenopathy may be observed as well.
Mammography is highly sensitive and specific for breast cancer in men, but it should be used to complement the clinical examination. At present, not enough clinical data are available to determine whether the combination of imaging and clinical findings can replace biopsy for the diagnosis of palpable breast abnormalities in men. Ultimately, biopsy should be considered to diagnose male breast cancer because the findings of inflammation, gynecomastia, and fat necrosis can be similar.
False Positives/Negatives
Inflammation, gynecomastia, and fat necrosis may appear similar on mammograms; therefore, these condition can cause false-positive findings. Cases of carcinoma have been found by ultrasonography after they were obscured on previous mammograms by gynecomastia.
A partially circumscribed retroareolar mass in a male with suspicious microcalcifications; this is known breast cancer.
Findings on Ultrasonography:
A hypoechoic mass with irregular, ill-defined, or circumscribed margins may be observed on ultrasonography. With color flow imaging, vascular flow within the mass may be demonstrated.
Similar sonographic findings may be observed in gynecomastia or inflammation; therefore, ultrasonography alone is not a reliable method to distinguish male breast cancer from other etiologies.
Read More
1-Supernumerary Nipple,Accessory Nipple, Polythelia,Ectopic nipple, Extra nipple, Hyperthelia.
2- Usually develop along the course of the embryological milk lines, which run from the anterior axillary folds to the inner thighs, but may also occur in other sites.
Acrocyanosis of the hands and feet commonly seen in newborns.
Acrocyanosis: Bluish discoloration of the extremities (the hands and feet). Acrocyanosis is typically symmetrical. It is marked by a mottled blue or red discoloration of the skin of the fingers and wrists and the toes and ankles and by profuse sweating and coldness of the fingers and toes.
Acrocyanosis is caused by narrowing (constriction) of small arterioles (tiny arteries) toward the end of the arms and legs.
c. Atelectasis of the left lung because of a mucus plug
d. Pneumonia in the left lung
e. Atelectasis of the left lung because the ETT is too low
Correct Answer:
Atelectasis of the left lung because the ETT is too low
Explanation
There is opacification of the left hemithorax. There is a shift of the heart and mediastinal structures (i.e. the trachea) toward the side of opacification. This eliminates pleural effusion, pneumonia and pulmonary edema as possibilities. A tension pneumothorax will displace the heart and mediastinal structures away from the side of the pneumothorax but it will not cause complete opacification of the opposite lung. In addition, there should be no lung markings visible in the hemithorax which contains the pneumothorax. If you look carefully, you will see the markers on an endotracheal tube that extends into the right mainstem bronchus. Thus, only the right lung is being aerated and the left lung has become atelectatic.
Salter-Harris fractures are fractures through a growth plate; therefore, they are unique to pediatric patients. Several types of fractures have been categorized by the involvement of the physis, metaphysis, and epiphysis. The classification of the injury is important because it affects the treatment of the patient and provides clues to possible long-term complications. * Type I - fracture through the physis (widened physis) * Type II - fracture partway through the physis extending up into metaphysis * Type III - fracture partway through the physis extending down into the epiphysis * Type IV - fracture through the metaphysis, physis, and epiphysis -- can lead to angulation deformities when healing * Type V - crush injury to the physis
No validated rules have been formulated for the use of radiography in patients with suspected ligament injuries, but a decision tree can be used as a guide (Figure below). Although plain radiographs may be useful in the initial diagnosis of these injuries, magnetic resonance imaging (MRI) is becoming the preferred diagnostic method and is rapidly replacing other techniques as the study of choice for the evaluation of knee injuries. However, the routine use of MRI has been questioned because of its significant cost ($600 to $1,200) and the high accuracy of clinical examination in diagnosing some injuries.
A knee x-ray is only required for knee injury patients with any of these findings:
age 55 or over
isolated tenderness of the patella (no bone tenderness of the knee other than the patella)
tenderness at the head of the fibula
inability to flex to 90 degrees
inability to weight bear both immediately and in the casualty department (4 steps - unable to transfer weight twice onto each lower limb regardless of limping)
A 31-year-old Caucasian male is admitted to the hospital with a 10-day history lower extremities rash and hands and feet swelling. He had upper respiratory tract infection before his current symptoms started.
A biopsy of skin lesions at an outside hospital shows leukoclastic vasculitis. All his other laboratory results are normal, including ESR, CRP, UA, CBC, CMP.
He received Celecoxib (Celebrex) 200 mg po daily started 5 days ago.Past medical history was Negative.
Physical examination:
Afebrile,well-developed and well-nourished
Chest: CTA (B).
CVS: Clear S1S2.
Abdomen: Soft, NT, ND, +BS.
Extremities: edema of hands and feet , purpura of lower extremities.
Edema of hands and feet
Purpura and edema of lower extremities
CBC, CMP, UA, ESR, CRP are all normal.
X-rays of hands are normal.
the likely diagnosis:Henoch-Schönlein Purpura
test to help confirm the diagnosis:
IgA
ASO
Throat culture
GC/Chlamydia probe
Stool guaiac
Results:
IgA level was elevated: IgA 516 mg/dL (lower limit 78, upper limit 391). ASO was elevated but the the throat culture was negative. The rest of the tests were normal.
Rheumatology and ID consults confirmed the diagnosis of Henoch-Schönlein purpura.
On hospital day 2, the purpura and swelling started to resolve. The patient felt much better and was discharged home with Celecoxib (Celebrex) 200 mg po qd and follow-up with rheumatology in 3-4 weeks. He was scheduled to have UA and BMP at that time to monitor for development of HSP-related renal disease.
What did we learn from this case?
Henoch-Schönlein purpura (HSP) is a self-limited systemic vasculitis. It is characterized by 4 clinical syndromes:
1. Palpable purpura in the absence of thrombocytopenia or coagulopathy. Develops in 100% of patients.
2. Arthritis/arthralgia in 45-75% of patients. Second most common manifestation of HSP.
3. Abdominal pain in 50%, GI bleeding (often occult) in 20-30% of patients.
A 65-year-old man collapses and is brought into the casualty department. Chest X-ray shows an increase in the cardiothoracic ration but clear lung fields. He is found to have decreased arterial pressure, increased central venous pressure, and faint heart sounds .
What is the most likely diagnosis?
a) Cardiogenic shock
b)Mitral regurgitation
c) Pericardial tamponade
d) Pulmonary embolism
e) Ventricular septal defect
The correct answer is C
Explanation
Pericardial tamponade classically results in the acute cardiac compression triad of Beck, which consists of decreased arterial pressure, increased central venous pressure, and distant heart sounds . Although clearly pathognomonic for tamponade, Beck's triad occurs in only 10% of individuals with pericardial tamponade
To keep it cool during hot-weather exercise, keep these basic precautions in mind:
* Take it slow . If you're used to exercising indoors or in cooler weather, take it easy at first. As your body adapts to the heat, gradually increase the length and intensity of your workouts. If you have a chronic medical condition or take medication, ask your doctor if you need to take additional precautions.
* Drink plenty of fluids . Your body's ability to sweat and cool down depends on adequate rehydration. Drink plenty of water while you're working out — even if you don't feel thirsty. If you're planning to exercise intensely or for longer than one hour, consider sports drinks instead. These drinks can replace the sodium, chloride and potassium you lose through sweating. Avoid drinks that contain caffeine or alcohol, which actually promote fluid loss.
* Dress appropriately . Lightweight, loosefitting clothing promotes sweat evaporation and cooling by letting more air pass over your body. Avoid dark colors, which can absorb the heat. A light-colored hat can limit your exposure to the sun.
* Avoid midday sun . Exercise in the morning or evening — when it's likely to be cooler outdoors — rather than the middle of the day. If possible, exercise in the shade or in a pool.
* Wear sunscreen . A sunburn decreases your body's ability to cool itself.
* Have a backup plan . If you're concerned about the heat or humidity, stay indoors. Work out at the gym, walk laps inside the mall or climb stairs inside an air-conditioned building.

 Axial CT in a patient without avascular necrosis of the femoral head shows prominent and thickened but normal trabeculae (arrow) within the femoral head. Note the delicate, sclerotic, raylike branchings emanating in a radial fashion from the central dense band. This is the asterisk sign.
Axial CT in a patient without avascular necrosis of the femoral head shows prominent and thickened but normal trabeculae (arrow) within the femoral head. Note the delicate, sclerotic, raylike branchings emanating in a radial fashion from the central dense band. This is the asterisk sign. Avascular necrosis, femoral head. Anteroposterior view of the pelvis shows flattening of the outer portion of the right femoral head from avascular necrosis (arrow), with adjacent joint space narrowing, juxta-articular sclerosis, and osteophytes representing degenerative joint disease.
Avascular necrosis, femoral head. Anteroposterior view of the pelvis shows flattening of the outer portion of the right femoral head from avascular necrosis (arrow), with adjacent joint space narrowing, juxta-articular sclerosis, and osteophytes representing degenerative joint disease. Avascular necrosis, femoral head. Coronal T1-weighted MRI in a patient showing hypointense signal within the proximal femoral neck and intertrochanteric regions (arrows) representing hematopoietic marrow. Increased signal is present within the greater trochanters and femoral capital epiphysis representing normal fatty marrow .
Avascular necrosis, femoral head. Coronal T1-weighted MRI in a patient showing hypointense signal within the proximal femoral neck and intertrochanteric regions (arrows) representing hematopoietic marrow. Increased signal is present within the greater trochanters and femoral capital epiphysis representing normal fatty marrow .